
Here’s How To Leverage Data for Health Equity
Healthcare Management, Health Policy Transformation, Health, Health Equity, Data & Analytics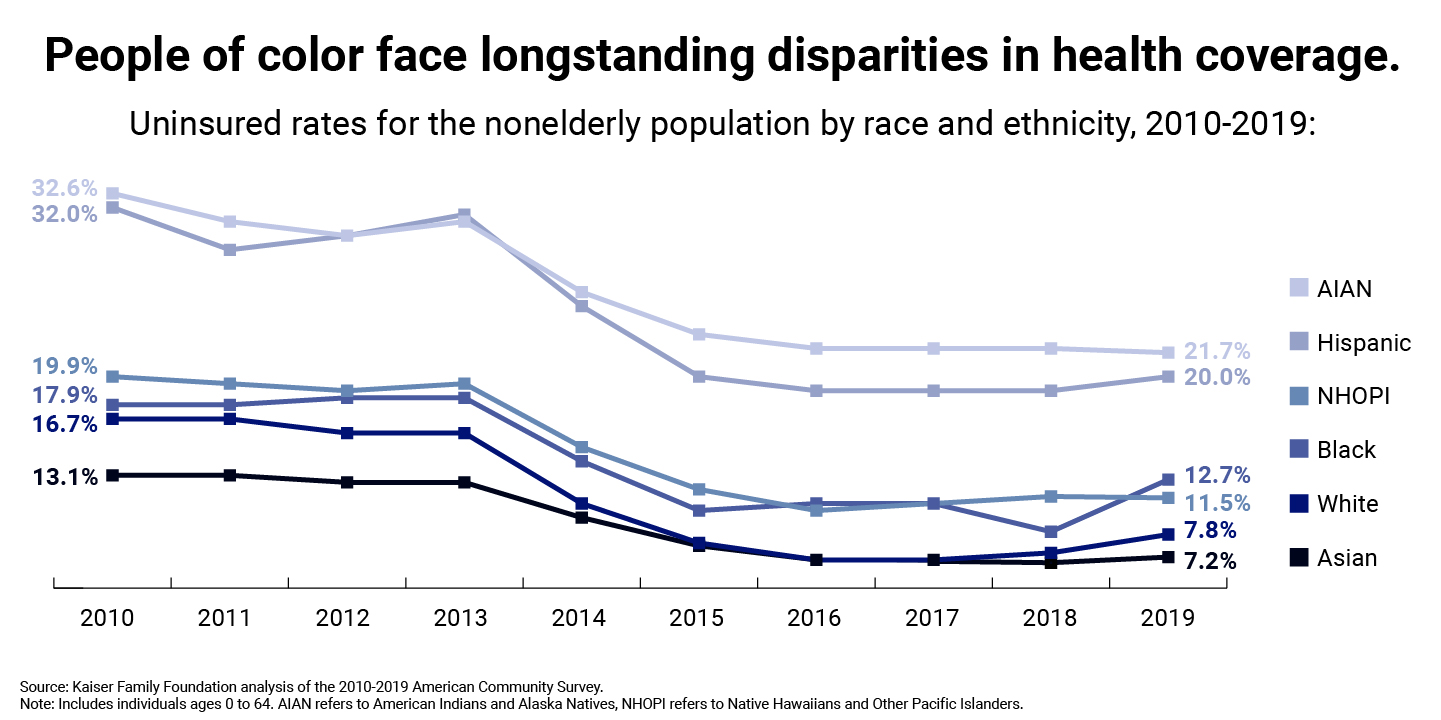
As the country grapples with the COVID-19 pandemic, the Biden administration is shining a spotlight on disparities in health and barriers to equity in the healthcare system. In a series of executive orders, the president called on all federal agencies to advance racial equity, support to underserved communities, and equitable pandemic response while charging the Centers for Medicare & Medicaid Services (CMS) and the Department of Health and Human Services (HHS) to work with providers and insurers to improve healthcare access and outcomes. These executive orders direct stakeholders to consider health equity and how the social determinants of health—including race, gender, geographical area, and income—affect interactions with the healthcare system.
The executive orders put significant federal weight behind understanding and addressing the barriers many Americans face in accessing quality healthcare. They offer a chance to improve data collection and analysis, provider and payer incentives, and coordination with community organizations to supply stakeholders with a clear view of access gaps. The Presidential COVID-19 Health Equity Task Force’s Final Report and Recommendations emphasize many of these opportunities by highlighting data-driven decision-making, community-led solutions, and accountability among its priorities. In this article, LMI experts explore these themes and their role in promoting a more equitable American healthcare system.
Understanding Healthcare Equity
Health equity is a state in which all people can live the healthiest lives possible. Achieving health equity means uncovering and removing the barriers to good health, which are tightly linked to social, demographic, economic, or environmental factors. For equity to exist in healthcare, everyone must have access to quality care regardless of location, identity, income level, or other socioeconomic characteristics.
In the healthcare system, significant disparities occur across geography, education, race, culture, gender, and income—in terms of access to healthcare and other health-promoting resources as well as the health outcomes that result. Disparities in access can arise when health services are not distributed equitably. This inequity became a principal concern early in the COVID-19 vaccination campaign. But even when healthcare services appear to be available equitably across geographies and populations, barriers to equitable access can emerge from other drivers. CMS recently noted the importance of language and cultural competency in messaging to citizens about healthcare availability and options. Making information available in a variety of languages and promoting cultural awareness, including through fostering a representative health workforce, can improve trust in the healthcare system. Building a system to restore and create healthcare equity requires taking all these factors into account.
Setting the Data Standard: Equity by Design
A foundational step in designing a more equitable healthcare system is uncovering where inequities exist and under what circumstances they arise, using relevant data. The healthcare system, education system, U.S. Census, and other federal initiatives and programs already generate significant data for understanding the state of healthcare equity nationwide. However, much of this data is unstructured and unstandardized, with little information sharing across agencies.
The federal government can lead the way to establish an equity-promoting data infrastructure through an interagency inventory of available socioeconomic, demographic, health, and other relevant data and setting standards for information collection and sharing. With a federal directive, rich stores of information could become available to stakeholders for analysis. These data, combined with healthcare data, supply a solid base for understanding disparities in healthcare equity more comprehensively.
Moreover, an interagency inventory would highlight data gaps that need new, timely collection efforts at the program level. Patient data flows throughout a person’s access to the healthcare system. Signing up for insurance, visiting a practitioner, and making insurance claims all create patient data. These secured data typically include the basics of a person's health, medical history, and some financial information. Healthcare intake operations offer access points to building healthcare equity into the design by collecting disaggregated data focused not only on basic patient information but factors leading to disparities in care.
To collect equity data, intake processes can include questions about socioeconomic, environmental, or geographic factors affecting a patient’s access to care. Gathering these data would establish a necessary baseline for understanding the state of equity in value-based care programs, care reimbursements, and payments. Equity lenses can be applied to analysis of patient outcomes to understand where gaps in care exist or when disparities in outcomes could relate to outside factors, like patient income or environmental issues. Effective use of technologies, such as machine learning, can help stakeholders understand and model patient populations to find gaps in care.
"Healthcare.gov has illustrated the importance of observing how people decide which plans they choose as well as refining the information available about health insurance and services," explains Allison Crowley, HHS project manager and lead data analyst for the Medicare Advantage market at LMI. "Data analysis shows policymakers how they can change subsidies to reach more people. We can use access points to improve data collection by structuring forms to more readily enable analysis."
Equity can be included in this analysis. Healthcare.gov already supplies some information on geographies and income. These data, combined with data from the census, can fill in details for insights about the decisions that citizens make when choosing insurance plans. Those insights can inform additional questions for study.
The healthcare system has significant opportunities to improve data entry. "Patient data or insurance claims data have significant gaps," explains Courtney Wright, a project manager for health policy and operations at LMI. "Insurers can take 30, 60, 90, or 120 days to file claims, creating a barrier to analysis because of the significant lag. Guidelines may differ state to state, which makes developing broad models of services use difficult.” Additional data collection points—like those from patients who self-pay—are even more fragmented. “At all these points, more standardization would make the data better and, ideally, faster to collect," states Wright.
Standardizing the data collected throughout intake and claims makes analysis of patient populations easier. Shortening the timeline for insurers to submit claims can improve tracking of patient outcomes as well as understanding of how and when the healthcare system is used.
Reinforcing Partnerships with Community Organizations
Due to historical events, marginalized groups may distrust the federal government and healthcare providers, making these groups hesitant to share data. To cultivate trust, the federal government and healthcare providers must keep patient data secure. In addition, though, many community organizations may already collect this information or have an awareness of disparities in equity in their localities and can be valuable sources of information and trusted organizations that reach out to citizens.
Healthcare conversation and debate often focuses on policies for affordability and quality of insurance. But attention should be paid to a growing number of community organizations offering essential services that, if supported, can improve access to care and information sharing. Community clinics, urgent care centers, and organizations, such as Meals on Wheels, serve as people’s access points for basic care. With greater federal support, these organizations can act as vital connections between underserved populations and the greater healthcare system.
"For many elderly people, organizations like Partners in Care or USAging could be a bridge," explains Michael Kelsey, healthcare program manager at LMI. "These organizations can alert care providers if something happens that requires medical or other attention, and they are repositories of data for harder to reach populations."
Working with community organizations can enable them to offer services to more people and create access points for underserved and hard-to-reach populations. These organizations have often served their communities for a long period and can supply valuable feedback to stakeholders on gaps in access and services, which feeds more equitable healthcare design. In addition, liaising with community organizations cultivates trust with marginalized groups and encourages their transparency for sharing personal medical history and data. Community organizations offload pressure from the broader healthcare system by working with people on non-emergency—but still important—issues, such as general wellness, nutrition, shelter, and concerns affecting overall health over time.
Promoting Equity in Payment and Incentives
As the largest single payer for healthcare in the United States, the federal government exerts huge influence on the healthcare system. The government’s buying power is a critical lever for encouraging equitable healthcare access and provision.
Extending and improving access to high-quality healthcare can reduce health disparities among underserved groups while supporting the shift to value-based care by improving patient outcomes. As HHS seeks to promote value-based models of care, it can establish payment incentives to reward providers for positive results in healthcare equity—for example, increasing access, quality, patient experience, and health outcomes in traditionally underserved communities. CMS can continue to lead the way by developing additional healthcare quality metrics to incorporate more equity-focused outcomes and by supporting the creation and testing of reimbursement models to incentivize achievement against them. CMS’s Meaningful Measures Framework, with its goal of working with communities to promote best practices of healthy living, is one of many federal initiatives improving outcomes for all patients. Defining metrics and asking the right questions will aid all healthcare stakeholders in measuring improvement as we address systemic weaknesses. In fact, the CMS Innovation Center released a strategy refresh with a stated aim to “embed health equity in every aspect of CMS Innovation Center models and increase focus on underserved populations.”
CMS can further its mission of providing high-quality healthcare at lower costs to more Americans, as expanding access to healthcare gives more people the opportunity to live their healthiest lives. Data-driven decision-making is critical to fulfilling this mission from an equity perspective. CMS uses data to assess the adequacy of provider networks in offering access to beneficiaries of public health insurance programs like Medicare. Stratifying these analyses by demographic and economic factors can reveal the extent to which such programs reach the most vulnerable and traditionally underserved, generating insights to improve healthcare equity.
Much can be done to improve healthcare equity in the U.S. By creating a strong foundation through data collection, standardization, and analysis with an equity lens, community outreach, and equity-centered incentives, leaders can build more equity into the system and improve access to care.


